
 Presented at the Academy of Breastfeeding Medicine Annual Meeting. Atlanta, GA, November 2017.
Presented at the Academy of Breastfeeding Medicine Annual Meeting. Atlanta, GA, November 2017.
Alison M. Stuebe1,3, Bharathi Zvara3, Samantha Meltzer-Brody2, Brenda Pearson2, Cheryl Walker2, Karen Grewen2
1Department of Obstetrics and Gynecology, 2Department of Psychiatry, 3Department of Maternal and Child Health,
Gillings School of Global Public Health, University of North Carolina, Chapel Hill, North Carolina
Background: Adverse childhood experiences are associated with mood disorders and difficulties with early caregiving behaviors. We sought to quantify associations among moderate/severe childhood trauma (MSCT), depression symptoms and breastfeeding intensity.
Methods: Women intending to breastfeed were recruited in the 3rd trimester of pregnancy for an ongoing longitudinal study. Past or current major depressive disorder or anxiety disorders were assessed via Structured Clinical Interview. Trauma history was quantified using the Childhood Trauma Questionnaire. MSCT was quantified using CTQ subscale scores (abuse: emotional≥13, physical≥10, sexual≥8; neglect: emotional≥15, physical≥10). During monthly interviews, mood was assessed via the Edinburgh Postnatal Depression Scale, and breastfeeding intensity in the past 7 days was assessed via a feeding questionnaire. Mean breastfeeding intensity and EPDS scores over the first 6 months and from birth to 12 months were used to calculate cumulative breastfeeding intensity (CBI) and cumulative EPDS (CEPDS). We used Wilcoxon rank sum tests to quantify the association between MSCT and CBI, and we used linear regression to model associations between CBI and CEPDS. P values <.05 were considered statistically significant.
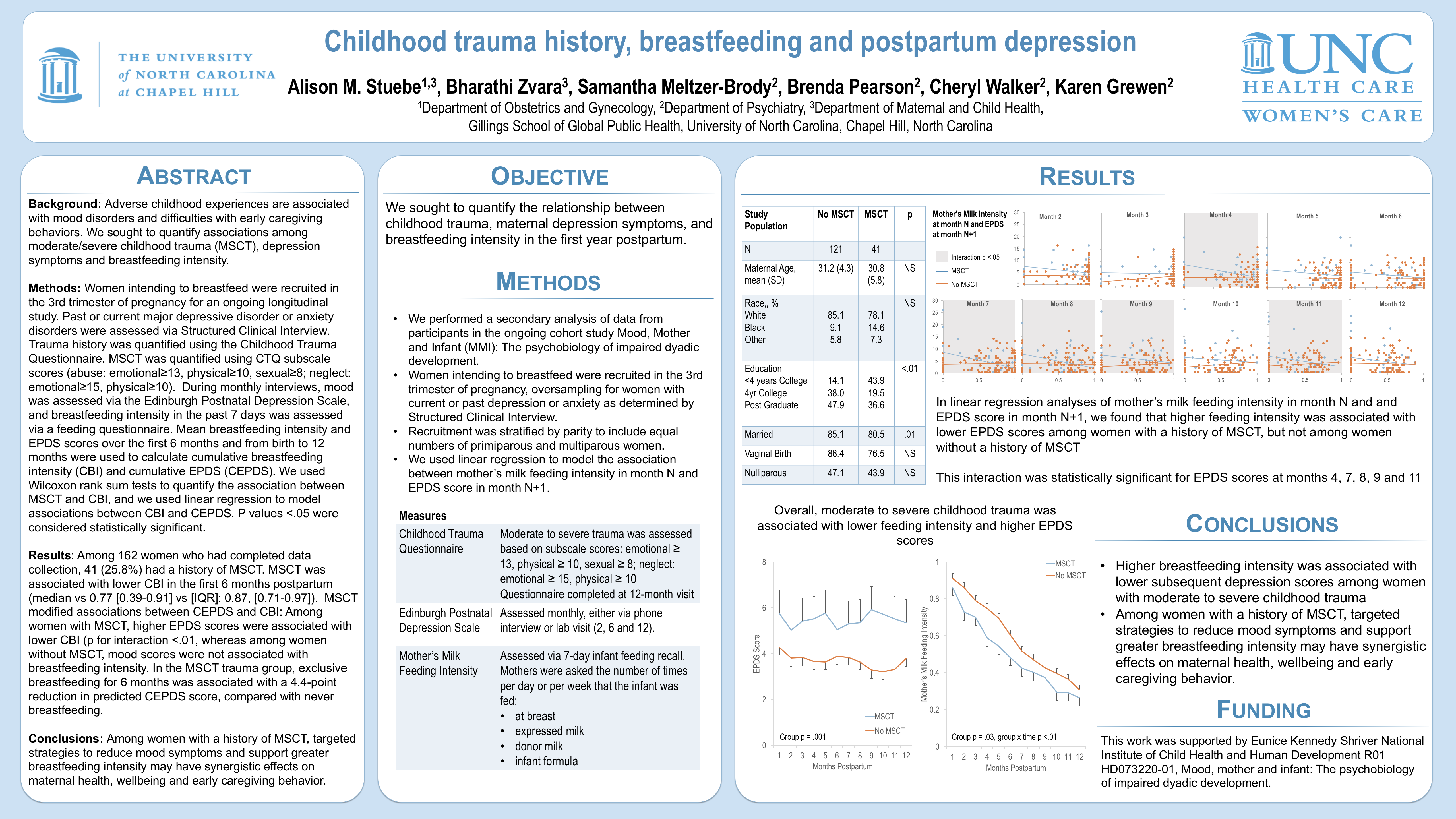
Results: Among 162 women who had completed data collection, 41 (25.8%) had a history of MSCT. MSCT was associated with lower CBI in the first 6 months postpartum (median vs 0.77 [0.39-0.91] vs [IQR]: 0.87, [0.71-0.97]). MSCT modified associations between CEPDS and CBI: Among women with MSCT, higher EPDS scores were associated with lower CBI (p for interaction <.01, whereas among women without MSCT, mood scores were not associated with breastfeeding intensity. In the MSCT trauma group, exclusive breastfeeding for 6 months was associated with a 4.4-point reduction in predicted CEPDS score, compared with never breastfeeding.
Conclusions: Among women with a history of MSCT, targeted strategies to reduce mood symptoms and support greater breastfeeding intensity may have synergistic effects on maternal health, wellbeing and early caregiving behavior.
